Therapy Techniques
The following techniques are used in dysphagia therapy to assist with those with anorexia and bulimia.
Nasogastric Tube

(Ask a Bipolar , 2011)
When weight loss from anorexia has been rapid or severe (more than 25% below ideal body weight), restoring body weight is crucial. Because such weight loss can be life-threatening, the individual is usually hospitalized so that experienced staff members can firmly but gently encourage the individual to eat. If unsuccessful, the individual may have to be fed intravenously or through a tube inserted in the nose and passed into the stomach. This is called a Nasogastric feeding tube or an "NG-tube." This procedure can be voluntary but if the patient is severely malnourished and refusing to eat and refusing a NG-tube then under the Mental Health Act (5150 involuntary psychiatric hold) they could be restrained and forced to have a NG-tube so that they can regain adequate nutrition (Ask a Bipolar , 2011). This technique would be ideal for someone struggling with anorexia. This technique along with the below mention
Nasogastric Intubation Demonstration Video
(Hobokiwi, 2008)
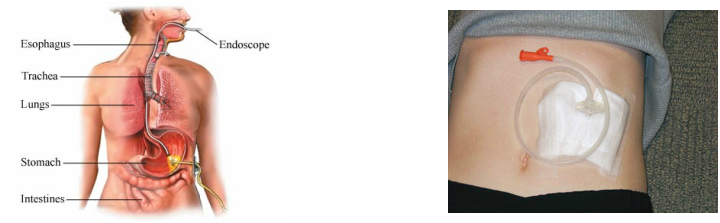
Percutaneous Endoscopic Gastrostomy
A Percutaneous Endoscopic Gastrostomy tube or a PEG tube is inserted through a small incision in the abdomen into the stomach (MD Guidelines, 2010). The surgeon inserts a needle into the stomach at the spot where the PEG tube will be located. Using the endoscope, the gastroenterologist locates the end of the needle inside the body, and encircles it with a wire snare. A thin wire is then passed from the outside of the body, through this needle and into the abdomen. This wire is then grasped with the snare and pulled out through the mouth. Now, there is a thin wire entering the front of the abdomen into the stomach and continuing upward and out the mouth. The PEG feeding tube is attached to this wire outside of the mouth. The surgeon then pulls the wire back out from the abdomen, which pulls the PEG down into the body through the mouth and esophagus. The tube is pulled until the tip of the PEG comes out of the incision in the stomach. There is a soft, round "bumper" attached to the portion of the PEG that remains inside the body, this bumper secures the tube on the inside of the body. The outer portion of the tube is secured with a bumper as well. Sterile gauze is placed around the incision site and the PEG tube is secured to your abdomen with tape (Muscular Dystrophy Australia, 2012). This technique would be ideal for someone struggling with anorexia.
This technique along with the NG tube mentioned above can be used to get an individual healthy enough to work on eating solid foods. Some individuals with anorexia develop a fear of swallowing (phagophobia) This could be a result of a traumatic event or the anxiety they experience about food and their weight which is associated with their disorder. Therefore a Speech Language Pathologist may have to suggest a PEG or NG tube first before working on dysphagia therapy which would get them healthy again while they gradually begin eating solid foods again (Schwartz, 2010). Individuals starting out on an NG tube or a PEG tube gain more weight weekly than with oral feeding and no tube which proves this method to be effective at aiding the individual to get healthier again (Zuercher JN, 2003).
This technique along with the NG tube mentioned above can be used to get an individual healthy enough to work on eating solid foods. Some individuals with anorexia develop a fear of swallowing (phagophobia) This could be a result of a traumatic event or the anxiety they experience about food and their weight which is associated with their disorder. Therefore a Speech Language Pathologist may have to suggest a PEG or NG tube first before working on dysphagia therapy which would get them healthy again while they gradually begin eating solid foods again (Schwartz, 2010). Individuals starting out on an NG tube or a PEG tube gain more weight weekly than with oral feeding and no tube which proves this method to be effective at aiding the individual to get healthier again (Zuercher JN, 2003).
(Muscular Dystrophy Australia, 2012)
(MD Guidelines, 2010)
Percutaneous Endoscopic Gastrostmy Placement Video
(FlocareTubes, 2009)
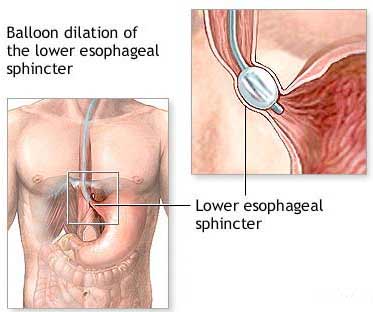
Esophageal Dilation
Esophageal stricture involves abnormal narrowing of the distal portion of the esophagus (American Society for Gastrointestinal Endoscopy , 2011). Symptoms of this disorder vary and may include difficulty swallowing (dysphagia), painful swallowing, regurgitation of food and weight loss (EndoNurse, 2004). There are a number of distinct causes of esophageal stricture. The most common is thought to be reflux esophagitis, in which prolonged exposure to stomach acid and peptic juices injures the esophagus, causing inflammation and scarring such as one with Bulimia would experience (American Society for Gastrointestinal Endoscopy , 2011). Esophageal dilation aids in the healing of esophageal stricture. There are two types of esophageal dilation the first of which involves inflating a balloon. Once the balloon has been inflated to the desired diameter, it is kept in place for a short time (30 seconds- 2 minutes) before deflating it. Then the balloon is taken out and an endoscope is used to look to see what effect it had—did it dilate, how much bleeding is there, and did it cause a perforation, which is always a risk. A second type of dilation involves the use of bougies, or savaries, which are rigid rubber tubes. Progressively larger bougies are passed through the mouth and down the esophagus using a wire in order to dilate the stricture. The lack of an endoscope during bougie dilation can be a disadvantage. It is not done under any direct visualization, but it may be done under fluoroscopy, where you would see a shadow in the X-ray (EndoNurse, 2004). This technique would be ideal for someone struggling with bulimia.
Most individuals with esophageal dysphagia have a nonobstructing esophageal lumen. The role of esophageal dilation in improving esophageal dysphagia with nonobstructive esophageal lumen is not clear; however, it did seem to show minimal improvement in individuals with more mild damage to their esophagus (Lavu K, 2004). Speech Language Pathologists could use this therapy to aid in expanding the esophagus of an individual with bulimia. The stomach acid that coats the esophagus after vomiting is the same acid that causes heart burn and other dysphagia related vomiting therefore causing the same type of irritation that narrows the esophagus. This technique allows the SLP to expand the esophagus so that the individual will find it easier to swallow food. On the road to recovery an individual with bulimia may find eating painful or difficult because of the damage the stomach acid has done over time to their esophagus.
Most individuals with esophageal dysphagia have a nonobstructing esophageal lumen. The role of esophageal dilation in improving esophageal dysphagia with nonobstructive esophageal lumen is not clear; however, it did seem to show minimal improvement in individuals with more mild damage to their esophagus (Lavu K, 2004). Speech Language Pathologists could use this therapy to aid in expanding the esophagus of an individual with bulimia. The stomach acid that coats the esophagus after vomiting is the same acid that causes heart burn and other dysphagia related vomiting therefore causing the same type of irritation that narrows the esophagus. This technique allows the SLP to expand the esophagus so that the individual will find it easier to swallow food. On the road to recovery an individual with bulimia may find eating painful or difficult because of the damage the stomach acid has done over time to their esophagus.
(American Society for Gastrointestinal Endoscopy , 2011)
Esophageal Dilation Videos
(Emedtv, 2009)
(Murrasaca, 2007)
Artificial Saliva
Anorexia and bulimia can often lead to dry mouth (xerostomia). This can greatly affect the individual's teeth, swallowing ability, and cause sores in the mouth and on the tongue. Therefore artificial saliva is recommended. Artificial Saliva acts just as regular saliva by cleansing and protecting the teeth and aiding in swallowing. Products are available in an aerosol or a liquid that is squirted into the mouth (American Dental Association, 2012). Saliva coats, lubricates tissues, helps cleanse the mouth, and begins the digestive process as one chews. Artificial saliva is not a perfect substitute for natural saliva because natural saliva is very complex physically and chemically. However it can help moisten the oral tissues, and relieve discomfort caused by dry mouth. Speaking, chewing, and swallowing all require saliva and become easier to do when the mouth is moist (American Dental Association, 2012). In dysphagia therapy an SLP could use artificial saliva to aid in chewing and swallowing for an individual suffering from dry mouth due to anorexia or bulimia. The American Dental Association approved artificial saliva as an effective technique to relieve dry mouth (American Dental Association, 2012). It however does not protect the teeth against acid erosion like natural saliva does so the individual should drink plenty of water and brush their teeth frequently with a toothpaste that protects enamel and reduces tooth sensitivity (Xiaojie Wang, 2011).

(Moss, 2011)
Artificial Saliva Videos
(AmericanDentalAssoc, 2011)
(MouthsMadeGood, 2010)
